Munchausen syndrome
Munchausen syndrome is an older term for a form of factitious disorder in which a person intentionally produces, fakes, or exaggerates physical or psychological symptoms to assume the patient role. The Diagnostic and Statistical Manual of Mental Disorders (DSM-5) classifies similar presentations under “Factitious disorder imposed on self,” characterized by deceptive behavior without obvious external incentives that would define malingering. The behavior may involve falsifying medical histories, tampering with tests or specimens, self-inflicted injuries, or fabricating symptoms across multiple settings and clinicians.

Munchausen syndrome (factitious disorder imposed on self) is a severe mental health condition where individuals deliberately fake, exaggerate, or induce physical or psychological illnesses in themselves to gain attention, sympathy, or the “patient” role. Symptoms include falsifying medical history, harming oneself, and manipulating tests. It is driven by deep-seated psychological factors and is difficult to treat.
Symptoms of Munchausen Syndrome
- Dramatic, inconsistent histories: Stories that change or don’t match medical findings.
- Fabricated symptoms: Claiming pain, fever, or seizures that cannot be verified.
- Self-harm: Inducing illness via infection, poisoning, or injury.
- Frequent hospitalizations: “Doctor shopping” across multiple hospitals.
- Unusual expertise: Extensive knowledge of medical terminology and hospital procedures.
- Willingness to undergo procedures: Seeking unnecessary tests or surgeries.
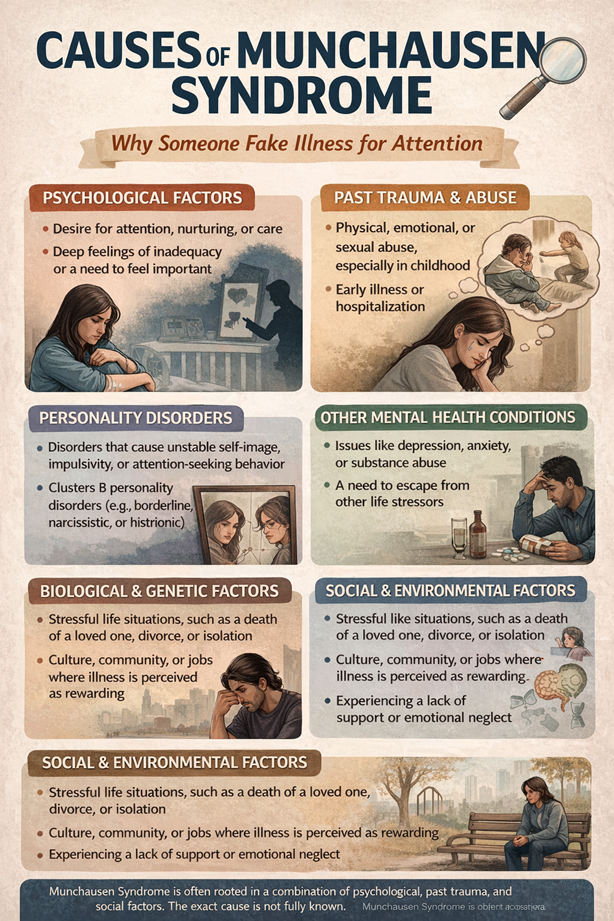
Causes and Risk Factors
The exact cause is unknown, but it is often linked to:
- Childhood trauma: A history of abuse, neglect, or abandonment.
- Early illness: A previous serious illness that garnered intense attention.
- Personality disorders: Underlying issues such as borderline or antisocial personality disorders.
- Unresolved issues: A need to punish oneself or be in control.
Prevalence and Complications
- Prevalence: Precise data is scarce because patients frequently move between doctors, making it challenging to track, though it is considered rare.
- Complications: Risks include severe organ damage from self-induced illnesses, surgical risks, chronic illnesses, and severe psychological distress.
- Mortality: In cases of Munchausen syndrome by proxy (where a child is the target), the mortality rate is estimated at 9%.
Related Conditions
- Munchausen Syndrome by Proxy (Factitious Disorder Imposed on Another): A caregiver, often a mother, makes a child ill to get attention.
- Munchausen by Internet: Fabricating illnesses in online support groups for sympathy.
Key Takeaways:
- Munchausen syndrome (a factitious disorder imposed on oneself) involves the deliberate production or feigning of physical or psychological symptoms to assume a sick role without obvious external incentives.
- Munchausen by proxy (factitious disorder imposed on another) involves a caregiver inducing or fabricating illness in someone else; this behavior is a psychiatric disorder and form of abuse, not an organic disease of the victim.
- Causes are multifactorial: prior abuse or neglect, early illness or hospitalization, personality disorders (often borderline or histrionic), strong need for attention or control, and sometimes learned medical knowledge.
- Clinical features include inconsistent or implausible histories, symptoms that do not match objective findings, frequent hospitalizations or provider hopping, eagerness for invasive tests or procedures, and resistance to psychiatric referral.
- Treatment emphasizes a nonjudgmental therapeutic alliance, targeted psychotherapy (CBT or psychodynamic approaches), management of comorbid psychiatric conditions, coordinated medical teams to limit unnecessary interventions, and legal/safeguarding actions when others are harmed.
- Hypnotherapy has limited and inconsistent evidence for factitious disorders; it may serve as an adjunct for comorbid trauma, dissociation, or somatic symptom relief but is not an established primary treatment.
- Prognosis is variable and often chronic with relapse risk; early detection, consistent care strategies, and protection for victims in by-proxy cases improve outcomes.
Investigation of Etiology and Pathogenesis of Munchausen Syndrome
Underlying psychological triggers and developmental factors
You encounter psychological drivers in what are the causes of munchausen syndrome that include early attachment disruption, histories of abuse or neglect, and repeated childhood hospitalization that teaches illness as a path to care.
Childhood medicalization and caregiver responses shape expectations; you may learn to equate sickness with attention and later adopt deceptive symptom production to secure care.
- Abuse or neglect in early years
- Prolonged hospitalization or medicalization
- Insecure attachment patterns
- Parental or caregiver illness modeling
- Personality disorder comorbidity (e.g., borderline personality disorder)
Attachment patterns and identity diffusion drive repeated presentations; when you need validation, you might fabricate symptoms to fill emotional voids. This pattern often resists standard therapeutic approaches.
Environmental influences on syndrome progression
Medical settings, clinician responses, and access to records influence progression; when you receive dramatic attention for fabricated symptoms, behavior can escalate and become more entrenched.
Healthcare fragmentation, frequent hospital admissions, and prior work in clinical roles give you routes to fabricate convincing presentations and to seek new facilities when challenged.
Social isolation, economic stress, and potential secondary gain from disability or litigation can maintain symptom production; community validation may unintentionally perpetuate the pattern.
Contextual influences such as media portrayals and online illness communities teach symptom mimicry and offer validation, which can accelerate recurrence and complicate treatment for you.
Diagnostic Indicators and Symptom Presentation for Munchausen Syndrome
When you evaluate a presentation, dramatic symptom reports, recurrent unexplained hospitalizations and inconsistent findings raise suspicion for Munchausen syndrome and Munchausen syndrome by proxy. You should watch for self-inflicted injuries, fabricated test results, or symptoms that appear only when the caregiver is present.
You will also note frequent medical language use, eagerness for invasive testing, and rapid escalation to procedures; Munchausen by proxy syndrome is not a disease but a behavior pattern often linked to complex psychological causes that require careful psychiatric assessment.
If you suspect fabrication, coordinate multidisciplinary review, compare records across institutions, and prioritize patient safety while arranging psychiatric referral and considering treatments ranging from psychotherapy to adjunctive hypnotherapy when clinically appropriate.
Identification of fabricated physical and psychological signs
While you inspect lesions, inconsistencies such as unusual wound patterns, inconsistent healing, or chemical burns should prompt toxicology screens and covert correlation with reported timelines.
As you evaluate psychological presentations, observe exaggerated symptom reports, dramatic affect shifts, knowledge of medical terms disproportionate to background, and signs of pseudologia fantastica indicating fabrication or rehearsal.
Through careful documentation and comparison to objective tests, you can distinguish true pathology from feigned symptoms, preserving the necessary treatment for genuine illness while limiting unnecessary interventions driven by fabricated reports.
Analysis of inconsistent medical histories and seeking behaviors for Munchausen syndrome
By tracking patterns of frequent hospital hopping, changing clinicians, and requests for repeat invasive testing, you will identify a behavioral profile consistent with Munchausen syndrome and potential Munchausen by proxy.
During interviews you should compare caregiver-reported timelines against medical records, lab results, and eyewitness accounts to reveal omissions, embellishments, or contradictions that undermine credibility.
Look for signs of wanting attention, rejecting normal explanations, and being very eager for medical procedures, as these can suggest deeper mental health issues that help guide decisions about referring for psychiatric help and considering treatments like hypnosis.
Recall that you must engage social services, ethics consultation, and legal safeguards when Munchausen by proxy is suspected. Use covert record review, multidisciplinary case conferences, and measured communication to protect vulnerable patients while arranging appropriate psychiatric care.
Comprehensive Treatment Approaches for Munchausen Syndrome
You should prioritize integrated care when considering treatments for munchausen syndrome, combining psychotherapies such as cognitive behavioral therapy, psychodynamic therapy, and dialectical behavior therapy with targeted pharmacotherapy for comorbid depression or anxiety (often SSRIs) and careful use of antipsychotics only when indicated by psychosis or severe dysregulation.
Clinicians must focus on building a consistent therapeutic alliance, using motivational interviewing and clear behavioral contracts to reduce deceptive presentations; you should limit unnecessary investigations and create agreed-upon care plans that steer management toward outpatient psychotherapy rather than repeated inpatient procedures.
Therapies are most effective when paired with system-level safeguards: you should involve liaison psychiatry, schedule regular outpatient follow-up, and implement relapse-prevention plans that monitor for recurrence of factitious behaviors while addressing underlying personality or trauma-related issues.
Multidisciplinary management and clinical protocols
Team composition typically includes psychiatry, psychology, primary care, nursing, social work, case management, and when relevant, ethics or legal consultants; you should ensure each member understands their role in coordinated treatments for munchausen syndrome and shares a single care plan.
Protocols should clearly outline how to prioritize cases, what needs to be recorded, and the time limits for getting psychiatric help (like consulting within 24-48 hours after identifying the issue); you need to keep track of previous consultations at different facilities, ensure informed consent is obtained, and set up alerts in the electronic medical record to avoid
Documentation practices require objective charts, photographic evidence only with consent, and behavioral contracts that outline limits on investigations; you should convene regular case conferences to review risk, adjust the care plan, and consider ethics review if deception leads to significant harm.
Long-term therapeutic goals and patient safety
Coordination aims to reduce frequency of factitious presentations and emergency visits by engaging you in sustained outpatient psychotherapy, strengthening coping skills, and treating comorbid diagnoses that maintain symptom production.
Goals include measurable targets such as fewer unplanned admissions, consistent attendance at weekly or biweekly therapy, and stabilization of mood or anxiety symptoms with medications like SSRIs when indicated; you should monitor progress with periodic outcome measures and modify treatments for munchausen syndrome accordingly.
Safety planning involves clear boundaries around invasive testing, scheduled access to care, family or caregiver involvement where appropriate, and a crisis plan that you can activate to prevent self-harm or medical harm resulting from fabricated symptoms.
Follow-up requires long-term engagement: you should schedule routine outpatient reviews, maintain a single primary clinician to reduce doctor-shopping, use written relapse-prevention agreements, and revisit the treatment plan every 3-6 months to sustain gains and protect patient safety.
Specialized Psychological Interventions for Munchausen Syndrome
Clinicians integrate targeted psychotherapies for factitious presentations, guiding you through structured contracts, boundary setting, and careful documentation to reduce iatrogenic harm and clarify treatment goals.
You will receive coordinated care pairing psychiatric assessments with medical teams, regular psychotherapy sessions, and risk-management plans tailored to persistent fabrication or symptom magnification.
Studies report multidisciplinary approaches reduce unnecessary procedures and hospital stays, and you should expect continuous outcome monitoring and consent-focused communication during interventions.
Homeopathic Treatments for Munchausen Syndrome
A person’s physical, emotional, and psychological problems are the main focus of homeopathic therapy. Homeopathic treatments for Munchausen Syndrome, a psychological disorder, focus on treating the underlying emotional and mental health problems rather than the dishonest behaviors.
Homeopathic RemediesHomeopathic Remedies

Ignatia: for patients who have experienced emotional trauma, loss, or neglect in the past. Ignatia reduces anxiety, violent emotional outbursts, and mood swings.
Natrum Muriaticum: For those who harbor intense melancholy and repress their feelings.
This remedy helps reduce reactivity to rejection or criticism.
Lachesis Mutus: beneficial for those with attention-seeking tendencies, jealousy, and excessive talkativeness. Lachesis may also alleviate feelings of neglect or hatred.
Stramonium: Best for people who act in an unpredictable, confused, or fearful manner. This homeopathic remedy helps people with a propensity to exaggerate and severe emotional disorders.
Arsenicum Album is for people who are worried about their hygiene and health. Arsenicum is Ideal for people who need comfort and are really nervous.
The application of hypnotherapy for munchausen syndrome
Hypnotherapy for munchausen syndrome appears in case reports as an adjunct to psychotherapy, where you may undergo 6-12 sessions using relaxation inductions and ego-strengthening suggestions to reduce urges to feign illness.
Patients receiving hypnotherapy often show decreased impulsivity and fewer emergency presentations, so you should track objective markers such as reduced invasive procedures and outpatient adherence over 3–6 months.
Therapists trained in clinical hypnotherapy combine trance work with cognitive restructuring, and you will need informed consent that addresses ethical risks, boundaries, and the adjunctive nature of this approach.
Cognitive and behavioral modification techniques
Cognitive techniques target distorted beliefs that sustain symptom fabrication, teaching you to identify automatic thoughts that justify deception and to test reality-based alternatives in session.
Behavioral modification techniques employ contingency management, activity scheduling, and graded exposure to illness cues so you practice non-sick-role behaviors and receive reinforcement for honest reporting.
Evidence from case series and small trials supports manualized CBT approaches, and you should expect 12–20 weekly sessions with routine outcome measurement to monitor reductions in factitious behavior.
Treatment frequently integrates motivational interviewing to address ambivalence, relapse-prevention planning tailored to your triggers, and family sessions to reduce secondary gain and repair relational patterns.
Final Words
Summing up, you should know Munchausen syndrome, now classified in DSM-5 as “Factitious disorder imposed on self,” takes its name from Baron Münchhausen (1720-1797) and involves deliberate production or feigning of symptoms to assume the sick role.
Causes are multifactorial, often including childhood abuse, comorbid personality disorders like borderline personality disorder, and relevant medical knowledge; core symptoms consist of fabricated histories, self-inflicted injuries, and repeated hospitalizations.
You should pursue coordinated care that emphasizes psychotherapy (cognitive behavioral therapy and long-term psychiatric follow-up management of comorbid depression or anxiety (for example, SSRIs), clear communication among clinicians, and careful risk assessment to avoid unnecessary procedures.
FAQ
Q: What is Munchausen syndrome?
A: Munchausen syndrome is an older term for a form of factitious disorder in which a person intentionally produces, fakes, or exaggerates physical or psychological symptoms to assume the patient role. The Diagnostic and Statistical Manual of Mental Disorders (DSM-5) classifies similar presentations under “Factitious disorder imposed on self,” characterized by deceptive behavior without obvious external incentives that would define malingering. The behavior may involve falsifying medical histories, tampering with tests or specimens, self-inflicted injuries, or fabricating symptoms across multiple settings and clinicians.
Q: What causes Munchausen syndrome?
A: No single cause explains factitious disorder; most clinicians view it as multifactorial with psychological, developmental, and sometimes biological contributors. Early-life experiences such as chronic childhood illness, inconsistent caregiving, trauma, or neglect can create patterns where illness becomes a means of obtaining attention or care. Personality disorders, especially borderline or histrionic traits, and co-occurring mood, anxiety, or substance use disorders increase risk. Psychological rewards such as increased attention, nurturance, or a sense of identity as a patient also help maintain the behavior.
Q: What are common signs and symptoms clinicians look for?
A: Presentation often includes inconsistent or dramatized symptom histories that do not fit objective findings, repeated hospitalizations with numerous diagnostic tests and procedures, eagerness for invasive interventions, and extensive medical knowledge or rehearsed details. Laboratory or clinical results that are difficult to reproduce, symptoms that appear only when the individual is observed by certain staff, or rapid improvement when care is withdrawn are red flags. Self-inflicted injuries, tampering with wounds or samples, and multiple aliases or frequent transfers between hospitals are additional warning signs.
Q: What is Munchausen by proxy and how does it differ from self-directed forms?
A: Munchausen by proxy, now termed “factitious disorder imposed on another,” involves a caregiver—most often a parent—who deliberately produces or fabricates illness in a person under their care, typically a child. The caregiver receives attention or sympathy by presenting the dependent as ill. The child or dependent experiences real medical harm even though the underlying illness is induced or falsified. Legal and child-protection systems treat this behavior as abuse rather than a medical disease in the victim, while the perpetrator is evaluated for psychiatric disorders.
Q: How is Munchausen syndrome diagnosed and distinguished from other conditions?
A: Diagnosis relies on careful, multidisciplinary assessment that rules out genuine medical and psychiatric disorders and documents intentional fabrication or induction of symptoms. Clinicians review prior records, obtain collateral histories, observe the patient across settings, and may repeat objective testing under controlled conditions. Distinction from malingering is based on motivation: factitious disorder involves internal psychological incentives to assume the sick role, whereas malingering involves external gains such as financial benefit or avoidance of responsibility. Ethical, legal, and safety factors dictate the necessity of covert surveillance or the engagement of protective authorities.
Q: What treatment approaches are available for Munchausen syndrome?
A: Treatment is challenging and centers on establishing a nonjudgmental therapeutic alliance, consistent care planning, and long-term psychiatric treatment. Psychotherapy is the core intervention; cognitive behavioral therapy and psychodynamic approaches can address maladaptive beliefs, interpersonal patterns, and past trauma. Management of co-occurring psychiatric conditions with evidence-based medications is often necessary. For factitious disorder imposed on another, priority actions include ensuring the safety of the victim, involving child protection or adult protective services, and coordinating medical and legal responses. Prognosis tends to be guarded, and sustained engagement with mental health services improves outcomes.
Q: Is hypnotherapy effective for Munchausen syndrome or Munchausen by proxy?
A: Evidence supporting hypnotherapy as a primary treatment for Munchausen syndrome consists mainly of case reports and small-series data. Hypnotherapy can help with dissociation, pain, or anxiety when used with psychotherapy, and it can be useful in trauma-focused care for some patients. Treatment of the caregiver in factitious disorder imposed on another rarely relies on hypnotherapy alone; safety planning and standard psychiatric interventions take precedence. Clinical decisions should be individualized and based on specialist input given the limited empirical support.
Hypnotherapy Treatment for Adjustment Disorder in Philadelphia
Philadelphia Hypnotherapy Clinic is the #1 hypnosis center in the city and suburbs. If you suffer from any form of emotional or behavioral disorder, including Munchausen syndrome and need hypnotherapy treatment, contact us at (267) 403-3085 or schedule an appointment for evaluation online. At the clinic, internationally recognized hypnotherapist and medical doctor Victor Tsan will perform one-on-one hypnotherapy sessions to create, embed, and develop positive synapses in your subconscious mind. You will experience something indescribable. The session usually lasts for almost 1.5 hours and will be your journey to heaven.