Trichotillomania—Hair-Pulling Disorder
There’s a condition you may not fully understand—trichotillomania, a hair-pulling disorder affecting approximately 1-2% of the population, often beginning in late childhood. You experience recurrent urges to pull out your hair, leading to noticeable loss and emotional distress. This guide outlines its causes, signs, and holistic ways to manage symptoms effectively.

Key Takeaways:
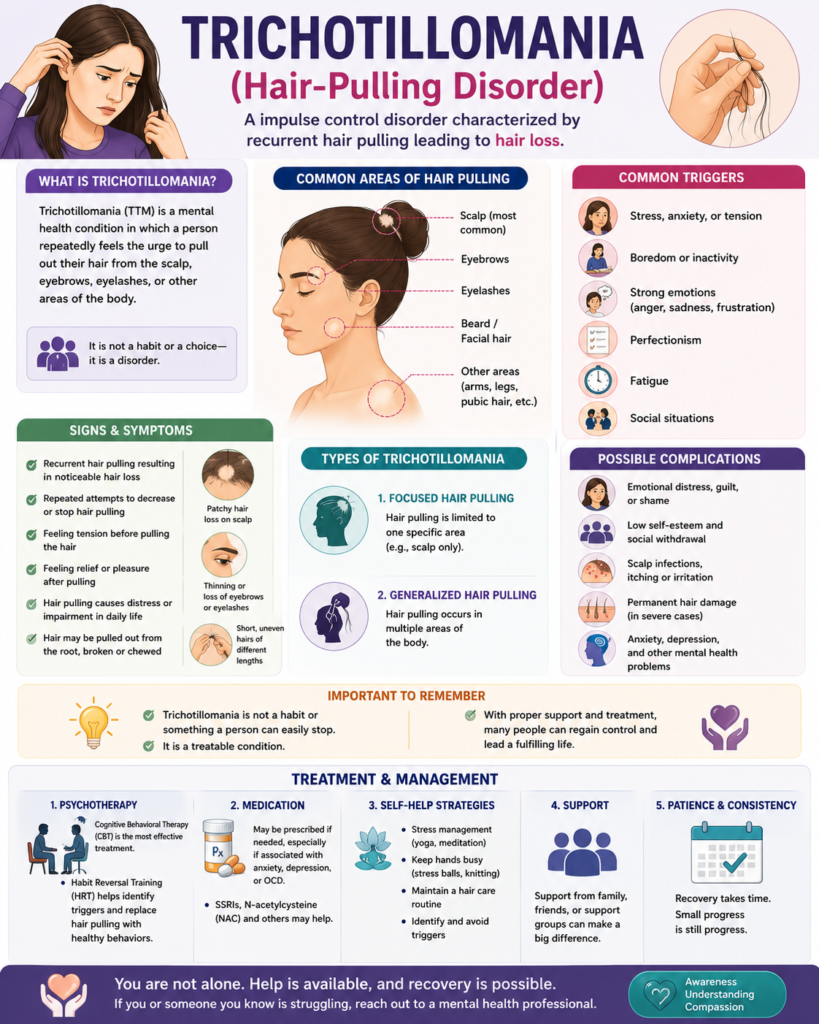
- Trichotillomania is a mental health condition characterized by recurrent, irresistible urges to pull out hair from the scalp, eyebrows, eyelashes, or other body areas, often resulting in noticeable hair loss.
- The exact cause of trichotillomania is not fully understood, but it likely involves a combination of genetic, neurobiological, and environmental factors, including stress, anxiety, and imbalances in brain chemicals like serotonin.
- Common triggers include emotional distress, boredom, fatigue, or sensory experiences such as feeling a particular hair texture, which can lead to unconscious or focused hair-pulling episodes.
- While trichotillomania shares some behaviors with obsessive-compulsive disorder (OCD), it is classified separately in diagnostic manuals as an impulse control disorder, though it can co-occur with OCD, anxiety, or depression.
- Physical complications may include skin irritation, infections, and in chronic cases, permanent hair loss or alopecia due to damage to hair follicles from repeated pulling.
- Standard treatments include cognitive-behavioral therapy (CBT), particularly habit reversal training, which helps individuals become aware of triggers and develop alternative responses to the urge to pull.
- Some people explore natural or complementary approaches such as acupuncture, hypnotherapy, or homeopathy, though scientific evidence for their effectiveness is limited and they should be used alongside evidence-based therapies.
Understanding Etiology and Environmental Triggers of Trichotillomania
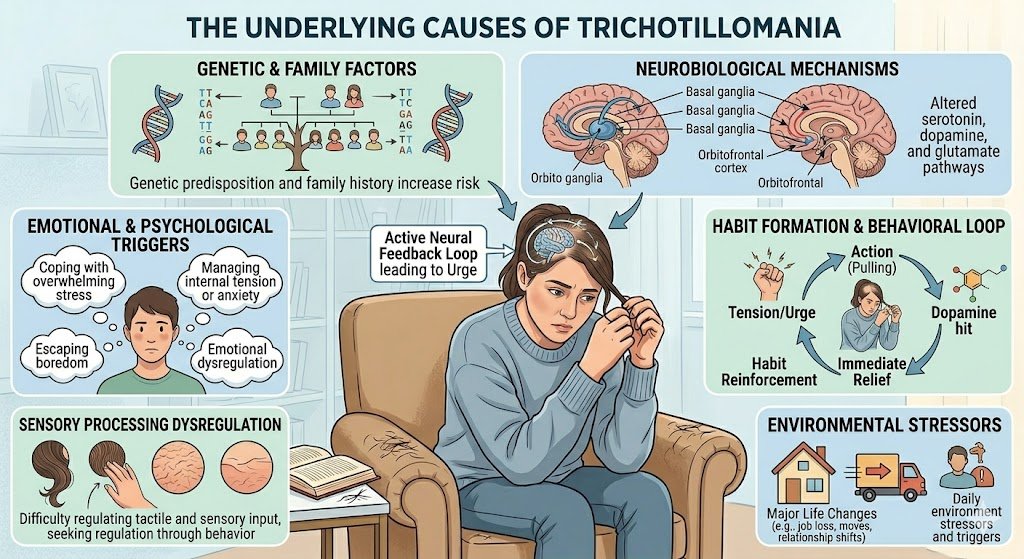
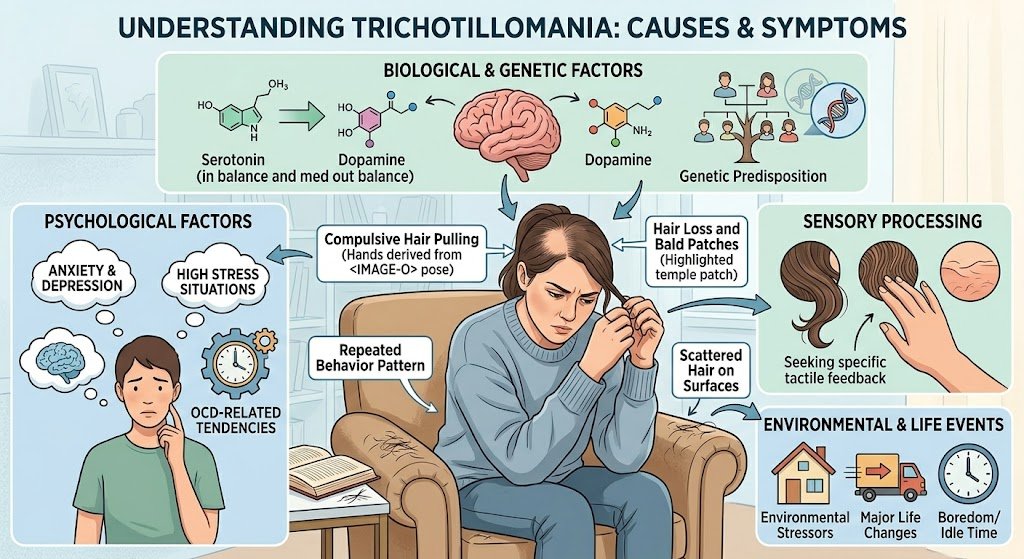
You may wonder what causes trichotillomania, a condition that affects approximately 1-2% of the population and has a higher prevalence in females. Research indicates it arises from a complicated interaction between biological, genetic, and environmental factors rather than a single origin. While no definitive cause has been isolated, neuroimaging studies show abnormalities in the frontal cortex and basal ganglia, brain regions involved in impulse control and habit formation. These neurological patterns suggest a dysfunction in motor inhibition, making hair-pulling behavior difficult to resist. Stress, anxiety, and emotional regulation challenges often act as key triggers for trichotillomania episodes. Many individuals report pulling more frequently during periods of heightened emotional distress, boredom, or fatigue. Environmental stressors such as academic pressure, family conflict, or traumatic life events—including abuse or loss—can initiate or worsen symptoms. Pulling may serve as a self-soothing mechanism, offering temporary relief despite long-term consequences.
Biological and Genetic Predispositions
Genetic studies reveal trichotillomania tends to cluster in families, with first-degree relatives showing a higher incidence. A 2006 study identified mutations in the SLITRK1 gene linked to trichotillomania in some individuals, suggesting a hereditary component. Neurotransmitter imbalances, particularly in serotonin and dopamine systems, further support a biological basis, mirroring patterns seen in obsessive-compulsive and related disorders.
Brain imaging shows structural and functional differences in individuals with trichotillomania, especially in the orbitofrontal cortex and anterior cingulate. These areas govern decision-making and impulse regulation, and their dysregulation may predispose you to repetitive behaviors. Twin studies indicate a heritability rate of up to 45%, reinforcing that biology plays a substantial role in vulnerability.
While no single gene determines onset, polygenic influences combined with neurodevelopmental factors increase risk. You may carry genetic markers that, when activated by environmental stressors, lead to symptom expression. This gene-environment interaction underscores why not everyone with a family history develops the condition.
Psychological Stressors and Emotional Catalysts
Emotional states like anxiety, frustration, or loneliness frequently precede hair-pulling episodes. You might pull without awareness during concentration or as a response to emotional discomfort, using the act to regulate mood. Childhood trauma, including emotional neglect or physical abuse, significantly increases risk, with studies showing up to 60% of individuals reporting adverse early experiences.
Stressful life transitions—such as moving, divorce, or academic failure—can trigger onset, particularly in adolescence. You may observe pulling intensifies during exams or interpersonal conflicts, suggesting emotional catalysts are central to symptom fluctuations. Cognitive distortions, like believing hair texture will change post-pull, further reinforce the behavior.
Even subtle emotional shifts, such as boredom or mild irritation, can prompt episodes. You might associate pulling with temporary relief, creating a cycle that’s difficult to break. Recognizing these emotional patterns is necessary for effective intervention.
Understanding the depth of psychological stressors reveals how trichotillomania is not merely a habit but a complex response to internal emotional states. You may experience shame or secrecy, which only deepens the cycle. Addressing these emotional catalysts through therapy—particularly cognitive-behavioral approaches—can lead to meaningful change by targeting the root emotional drivers, not just the surface behavior.
Clinical Manifestations and Symptomology of Hair Pulling Disorder
Repetitive hair pulling defines the core symptoms of trichotillomania, often leading to noticeable hair loss and emotional distress. You may experience an increasing sense of tension before pulling or when resisting the urge, followed by relief or gratification afterward. These patterns typically occur in private and can persist for minutes or hours, often without full awareness. The behavior is not due to another medical condition, such as alopecia, and must be distinguished from cosmetic grooming practices.
Many individuals report specific triggers, including stress, boredom, or sedentary activities like watching television or lying in bed. The onset commonly occurs in childhood or adolescence, with peak diagnosis between ages 10 and 13. Without intervention, symptoms of trichotillomania can become chronic, affecting social functioning, self-esteem, and daily routines. Some people may also engage in trichophagia—eating the pulled hair—which increases the risk of gastrointestinal complications like trichobezoars.
Diagnosis relies on clinical evaluation using criteria from the DSM-5, which requires recurrent hair pulling resulting in hair loss, repeated attempts to decrease or stop the behavior, and significant distress or impairment. Dermatological exams and patient history help rule out other causes. Awareness of these symptoms of trichotillomania enables earlier intervention and improves long-term outcomes.
Physical Signs and Identification of Pulling Patterns
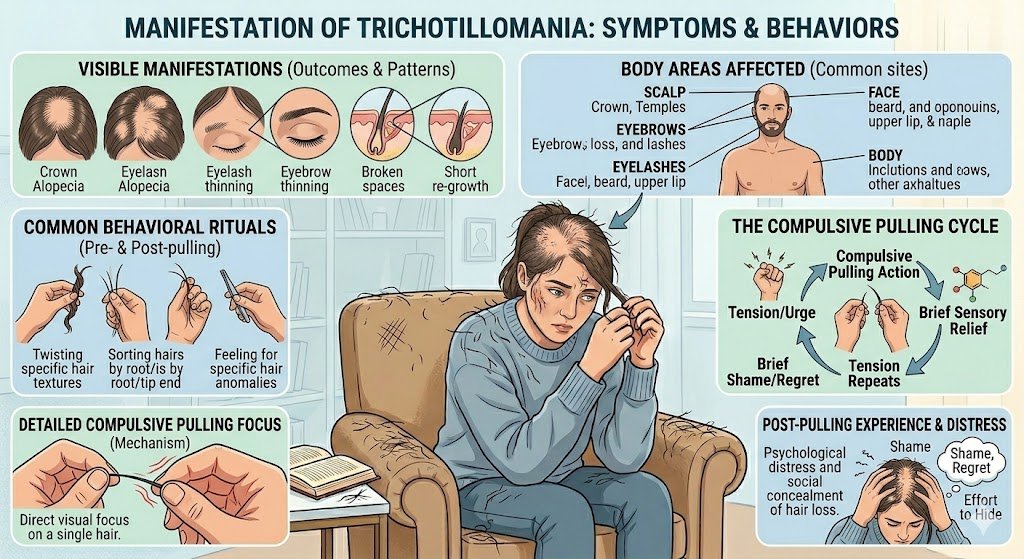
Irregular patches of hair loss with varying lengths of remaining strands often signal trichotillomania. You might notice broken hairs of different stages of growth, a hallmark sign distinguishing it from other forms of alopecia. These patterns are typically asymmetrical and avoid clean, geometric shapes, reflecting the unconscious, compulsive nature of pulling. Close inspection may reveal evidence of trauma to the follicles, such as erythema or scabbing.
Some individuals develop preferred pulling methods, using fingers, tweezers, or even teeth, which can leave subtle clues on the hair shafts. Trichoscopy, a non-invasive imaging technique, may reveal “exclamation mark” hairs or coiled structures consistent with mechanical damage. These physical markers help clinicians confirm diagnosis when self-reporting is limited or inconsistent.
Pulling frequency varies—some episodes occur automatically during distraction, while others are focused and ritualistic. You may pull more during sedentary tasks or at specific times of day. Recognizing these behavioral rhythms supports tailored treatment planning and increases the likelihood of sustained symptom reduction.
Targeted Areas: Impact on Eyebrows and Facial Hair
Eyebrows are among the most commonly affected sites in trichotillomania, with many individuals reporting frequent pulling from this area. You may experience thinning, patchy loss, or complete absence of eyebrow hair, which can significantly alter facial expression and self-perception. Unlike scalp hair, eyebrow regrowth is often slower and less dense, making the cosmetic impact more pronounced and distressing.
Facial hair, including eyelashes and beard areas, is also frequently targeted. Chronic eyelash pulling, known as trichotillomania when it specifically involves the eyebrows, can lead to ocular irritation, misdirected regrowth, or even corneal abrasions. The visibility of these areas intensifies feelings of embarrassment, prompting avoidance of social interactions or reliance on makeup and prosthetics to conceal damage.
Research indicates that up to 50% of individuals with trichotillomania report pulling from the eyebrows or eyelashes, emphasizing the necessity of targeted interventions. You may develop rituals around grooming these areas, mistaking the behavior for normal maintenance. Recognizing trichotillomania eyebrows as a clinical symptom—not a cosmetic issue—is crucial for effective treatment and emotional recovery.
When trichotillomania affects the eyebrows, the psychological toll often extends beyond appearance. You may feel hyper-aware of others’ gazes, interpret neutral expressions as judgmental, or withdraw from activities requiring face-to-face engagement. The loss of eyebrows—key elements in nonverbal communication—can disrupt social signaling, further isolating you. Treatment must address both the physical manifestations and the deep-seated emotional consequences to support lasting healing.
Psychological Classification and OCD Relationships with Trichotillomania
Trichotillomania, formally recognized in the DSM-5, is classified under obsessive-compulsive and related disorders, a grouping that reflects its behavioral and psychological overlap with conditions like OCD. While it was once considered an impulse control disorder, its reclassification in 2013 marked a significant shift in understanding its nature. You may notice repetitive behaviors in both trichotillomania and OCD, but the driving forces differ—trichotillomania often stems from urges tied to sensory regulation rather than obsessive thoughts.
Trichotillomania within the Obsessive-Compulsive Spectrum
Researchers like Dr. Dan Stein have long argued that trichotillomania belongs to an obsessive-compulsive spectrum due to shared features such as repetitive behaviors and difficulty resisting urges. You might pull hair in response to tension or anxiety, much like how someone with OCD performs rituals to relieve distress. However, unlike classic OCD, the act of pulling often brings a sense of relief or gratification, not just anxiety reduction.
This spectrum model, introduced by Dr. Eric Hollander in the early 2000s, includes disorders where compulsive behaviors dominate despite varying triggers. You may discover that hair-pulling episodes occur both consciously and automatically, with studies showing up to 75% of cases involving automatic pulling. This classification receives further support from the overlap in neurobiology—particularly in the cortico-striato-thalamo-cortical (CSTC) circuits.
Despite these links, trichotillomania is not OCD. You experience it differently: OCD involves intrusive thoughts driving rituals, while trichotillomania centers on the urge to pull, often without obsessive ideation. Recognizing this distinction helps shape more accurate treatment approaches and reduces misdiagnosis.
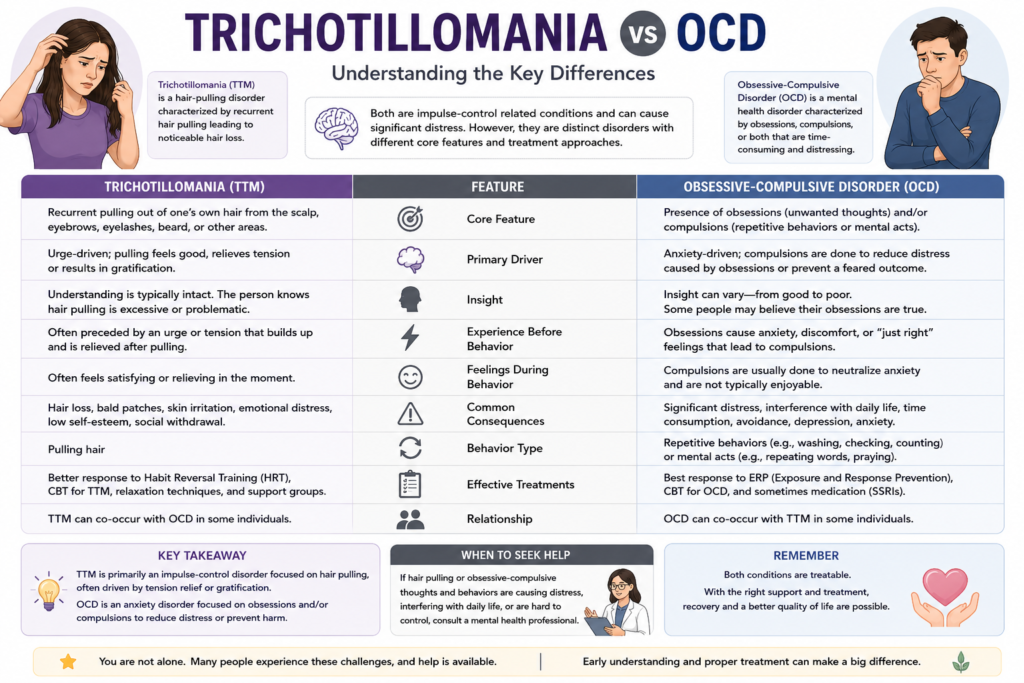
Comparative Diagnostic Criteria and Differences
Understanding how trichotillomania and OCD differ diagnostically clarifies treatment paths and patient experiences. You may meet DSM-5 criteria for trichotillomania if you repeatedly pull hair, leading to hair loss and repeated attempts to stop, without another medical cause. In contrast, OCD requires the presence of obsessions, compulsions, or both, consuming more than one hour daily.
These distinctions matter clinically. You might pull hair to relieve tension, not to neutralize a feared outcome like contamination. The table below outlines key differences based on DSM-5 criteria and clinical research:
Diagnostic Comparison: Trichotillomania vs. OCD
| Feature | Trichotillomania | OCD |
| Primary Behavior | Repetitive hair pulling | Compulsions (e.g., washing, checking) |
| Driving Force | Urge relief, sensory satisfaction | Anxiety reduction from obsessions |
| DSM-5 Classification | Obsessive-Compulsive and Related Disorders | Obsessive-Compulsive and Related Disorders |
| Onset Age (Average) | 12-13 years | 19-20 years (can be earlier) |
| Intrusive Thoughts Required? | No | Yes |
While both conditions fall under the same DSM-5 chapter, their mechanisms diverge significantly. You may struggle with shame and secrecy in both, but the absence of obsessions in trichotillomania means cognitive models used for OCD don’t always apply. Tailoring therapy to address urge regulation, not thought suppression, leads to better outcomes. Recognizing these nuances ensures you receive care aligned with your actual experience, not a misapplied label.
Long-Term Physical Complications of Hair Pulling Disorders
Chronic hair pulling in trichotillomania can lead to lasting physical consequences, especially when left untreated over years. You may notice thinning patches or complete bald spots on the scalp, eyebrows, or eyelashes, depending on your pulling patterns. These areas are not only cosmetically distressing but can also disrupt the natural hair growth cycle, leading to more serious dermatological issues.
Repeated trauma to hair follicles increases inflammation and scarring beneath the skin’s surface. You might develop folliculitis, a painful infection of the hair follicles, or experience skin abrasions that invite bacterial invasion. Without intervention, these conditions can worsen, particularly if you use unsterilized tools or pull with dirty hands.
Over time, persistent pulling can permanently damage hair follicles, leading to irreversible hair loss. You may be wondering, can trichotillomania cause alopecia? Yes, specifically, it can result in traction alopecia or even scarring alopecia when follicles are destroyed. Studies indicate that up to 40% of individuals with long-standing trichotillomania develop some degree of permanent alopecia, particularly in commonly targeted areas like the front and sides of the scalp.
Dermatological Damage and Infection Risks
Each time you pull hair, especially with force or using tweezers, you risk micro-tears in the skin. These tiny wounds may not seem serious, but they create entry points for bacteria like Staphylococcus aureus, increasing your chance of infection. Redness, swelling, and pus-filled lesions are common signs of folliculitis, a frequent complication in chronic cases.
You might also develop hyperpigmentation or hypopigmentation in affected areas, where the skin becomes darker or lighter due to repeated trauma. Scarring can occur beneath the surface even before it’s visible, compromising the skin’s elasticity and healing capacity. Dermatologists often observe lichen planopilaris-like changes in long-term patients, indicating ongoing inflammatory damage.
Infected lesions can escalate into abscesses or cellulitis if untreated, requiring antibiotics or medical drainage. You’re at higher risk if you pull from the same sites daily, as constant manipulation prevents proper healing. Keeping the skin clean and seeking early dermatological care can reduce these risks significantly.
Progression Toward Permanent Alopecia
Trichotillomania can absolutely lead to permanent hair loss when people pull their hair for years. You may start with temporary thinning, but over time, the constant trauma causes fibrosis—scar tissue replaces healthy follicles. Once this process happens, hair can no longer grow, resulting in irreversible alopecia.
Studies indicate that approximately 30-40% of individuals with trichotillomania develop permanent alopecia, particularly in high-tension areas like the frontal hairline. This condition is often diagnosed as scarring alopecia or pseudopelade, where biopsy reveals destroyed follicular structures. The longer the behavior continues, the higher the risk of permanent damage.
You might not notice the shift from reversible to irreversible loss immediately. Early signs include smooth, shiny patches with no visible follicular openings. Dermoscopy can detect changes before they’re visible to the naked eye, making early intervention critical. Once follicles are gone, treatments like hair transplants may be the only option.
Permanent alopecia from trichotillomania isn’t just about missing hair—it reflects years of physical trauma to delicate scalp tissue. You may experience psychological distress, compounded by visible scarring, which complicates treatment. However, stopping the pulling behavior can halt further damage, and dermatological therapies like corticosteroid injections or minoxidil may help in borderline cases where follicles are weakened but not fully destroyed.
Conventional and Natural Treatment Frameworks
Clinical Interventions and Behavioral Therapies for Trichotillomania
You may discover that trichotillomania treatments often begin with evidence-based behavioral therapies. The most widely supported approach is habit reversal training (HRT), a method first developed in the 1970s that helps you recognize triggers and replace hair-pulling with competing responses. Studies show that HRT leads to significant improvement in over 60% of patients when delivered consistently. Another effective option is cognitive behavioral therapy (CBT), which addresses distorted thoughts linked to the behavior. In some cases, clinicians prescribe medications like N-acetylcysteine (NAC), an amino acid supplement studied for its impact on impulse control. A 2009 trial by Grant and colleagues found that 56% of participants taking NAC reported reduced pulling compared to placebo. These clinical strategies form the foundation of most treatment plans.
Behavioral interventions work best when tailored to your specific patterns and emotional triggers. Dialectical behavior therapy (DBT) skills, such as distress tolerance and emotional regulation, are increasingly integrated into treatment for those with co-occurring anxiety or mood disorders. You might also benefit from acceptance and commitment therapy (ACT), which encourages mindfulness and values-based action instead of symptom suppression. Therapists often use functional analysis to map when, where, and why you pull, allowing for personalized strategies. With consistent practice, these therapies help rewire automatic behaviors and build long-term self-awareness.
Your progress depends not only on therapy type but also on treatment duration and support systems. Weekly sessions over 10 to 12 weeks are typical, though some require longer engagement. Telehealth platforms now offer access to specialists, increasing availability for those in remote areas. You’re more likely to succeed when therapists, family, and support groups collaborate. Clinical guidelines from the Trichotillomania Learning Center emphasize early intervention and multidisciplinary care. These structured approaches remain the most validated path toward managing trichotillomania symptoms effectively.
Integration of Natural Management Strategies for Hair Pulling Disorder
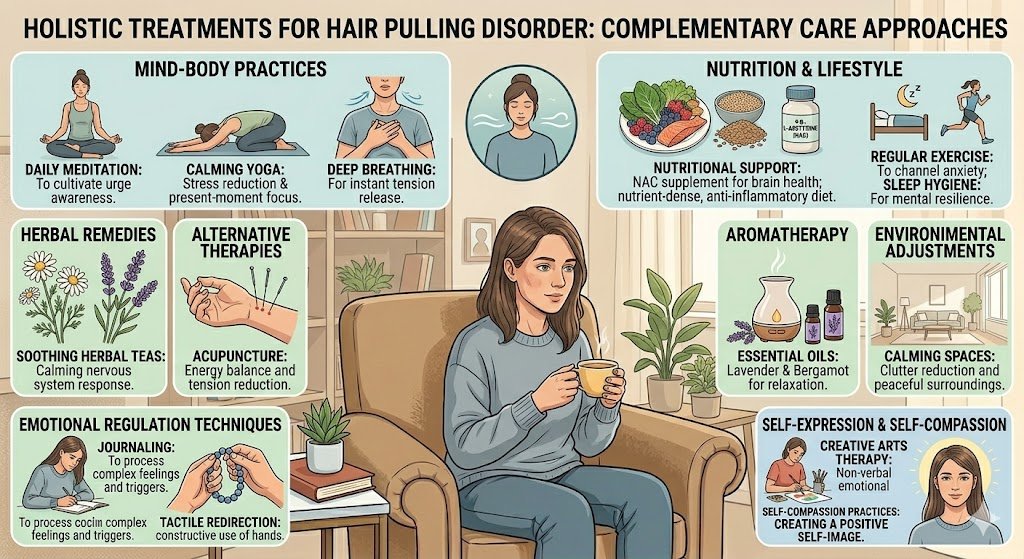
Many people explore natural treatment for trichotillomania to complement clinical care. You might consider dietary supplements like inositol, which showed promise in a 2013 pilot study where participants reported reduced urges after six weeks of use. Omega-3 fatty acids, known for anti-inflammatory and neurological benefits, are also used to support brain health and mood stability. Herbal remedies such as passionflower or valerian root may help manage anxiety, a common trigger. While not replacements for therapy, these natural options can play supportive roles when used under professional guidance.
Lifestyle adjustments often enhance your overall response to treatment. You may notice fewer urges when maintaining a consistent sleep schedule, practicing yoga, or engaging in tactile alternatives like fidget tools. Mindfulness meditation, practiced for 10 to 15 minutes daily, has been linked to decreased hair-pulling frequency in multiple case reports. Some find relief through acupuncture, though clinical evidence remains limited. The key is integrating these strategies intentionally, tracking their effects over time, and adjusting as needed.
Your journey may include trial and error as you identify which natural methods work best. Journaling your pulling episodes alongside supplement use or relaxation practices helps reveal patterns. You’re not alone—online communities and forums dedicated to natural treatment for trichotillomania share real-world experiences and practical tips. While scientific research on alternative approaches is still emerging, many report improved control when combining these methods with behavioral therapy. Always consult your healthcare provider before starting new supplements to avoid interactions.
Expanding on the Integration of Natural Management Strategies, you’ll find that consistency and personalization are central to success. Natural treatment for trichotillomania isn’t about quick fixes but building a sustainable, holistic routine. For example, pairing N-acetylcysteine—a supplement studied in trichotillomania treatments—with daily mindfulness practice may enhance impulse control more than either method alone. You might use textured bracelets or gloves to create physical barriers, reducing unconscious pulling. These strategies work best when aligned with your daily habits and emotional needs, making them easier to maintain long-term. The growing body of anecdotal and clinical evidence suggests that when natural approaches are thoughtfully layered with professional care, you stand a better chance of achieving meaningful symptom reduction.
Integrative and Mind-Body Therapies for Trichotillomania
Alternative Medicine: Acupuncture and Homeopathy for Hair-Pulling Disorder
Acupuncture for trichotillomania has been explored as a method to balance the body’s energy flow and reduce compulsive behaviors by stimulating specific meridian points. Some practitioners believe that inserting fine needles at key locations can regulate neurotransmitters linked to impulse control, potentially easing the urge to pull hair. While clinical trials remain limited, anecdotal reports suggest improvements in anxiety and hair-pulling frequency after consistent sessions.
Homeopathy for trichotillomania relies on highly diluted natural substances intended to stimulate the body’s self-healing mechanisms. Remedies like *Staphysagria* or *Arsenicum album* are often selected based on individual emotional profiles, such as irritability or perfectionism. Though scientific validation is sparse, some patients report reduced pulling episodes when integrating homeopathy into a broader treatment plan.
You may find that alternative approaches like acupuncture and homeopathy offer complementary support, especially when traditional therapies fall short. These methods focus on holistic balance rather than isolated symptoms, aligning with a personalized care model. Always consult a licensed practitioner to ensure safe integration with other treatments.
Cognitive Regulation: Hypnotherapy and Hypnosis Techniques for Trichotillomania
Hypnotherapy for trichotillomania uses guided relaxation and focused attention to access subconscious patterns driving hair-pulling behavior. During sessions, a trained therapist may introduce suggestions aimed at increasing self-awareness and replacing compulsive urges with healthier responses. Many patients report heightened control over impulses after several weeks of consistent practice.
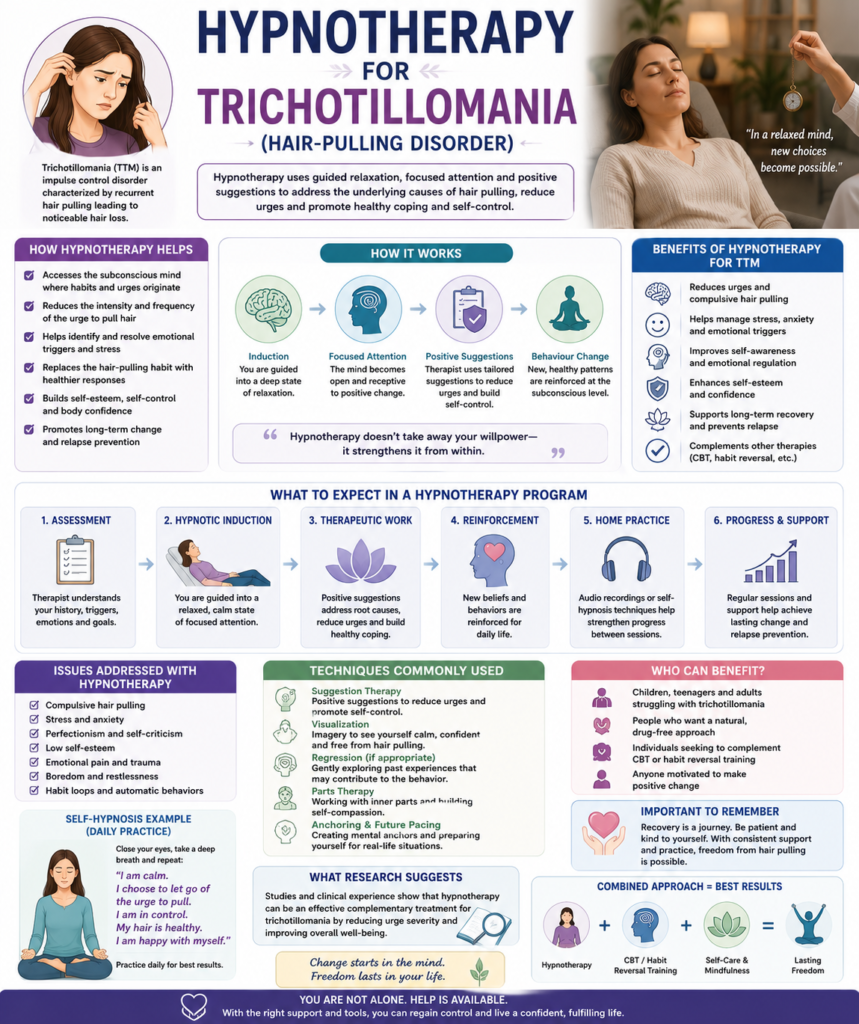
Hypnosis for trichotillomania often involves self-hypnosis techniques you can use daily to interrupt automatic pulling episodes. By rehearsing mental cues like “I choose to let my hair be,” you retrain your brain’s response to stress or boredom. Studies indicate that hypnosis can reduce pulling frequency, particularly when combined with cognitive-behavioral strategies.
This mind-body approach emphasizes your ability to influence unconscious habits through focused intention. Hypnotherapy and hypnosis for trichotillomania are non-invasive and adaptable, making them accessible options for long-term management. With regular practice, you may notice not only fewer pulling episodes but also improved emotional regulation.
Building on cognitive regulation, hypnotherapy and hypnosis for trichotillomania change automatic behaviors at a subconscious level. These techniques help you recognize internal triggers—like tension or distraction—and respond with mindful alternatives. Over time, this reprogramming supports lasting behavioral change without reliance on medication.
Final Words
Presently, trichotillomania is recognized as a complex mental health condition rooted in both biological and psychological factors. You may experience hair pulling due to imbalances in brain chemistry, genetic predisposition, or as a response to stress and anxiety. Triggers often include emotional distress, boredom, or habitual routines such as grooming. The disorder typically begins in childhood or adolescence, with studies showing onset most commonly between ages 10 and 13, and affects up to 4% of the population, with higher prevalence in females.
Holistic management offers a practical path forward by combining evidence-based therapies like cognitive behavioral therapy (CBT) and habit reversal training (HRT) with mindfulness, stress reduction, and lifestyle adjustments. You benefit from structured interventions that address both the behavior and its emotional underpinnings. Clinical trials indicate that over 60% of individuals show marked improvement with consistent CBT application.
Your long-term success depends on consistent self-monitoring, professional support, and compassionate self-awareness. Trichotillomania is not a matter of willpower but a treatable condition requiring patience and tailored strategies. By integrating medical guidance with mindful daily practices, you build sustainable control and improve overall well-being.
FAQ

Q: What is trichotillomania and what are its main symptoms?
A: Trichotillomania is a mental health condition characterized by a repeated urge to pull out hair from the scalp, eyebrows, eyelashes, or other body areas. People with this disorder often feel increasing tension before pulling or when trying to resist, followed by relief or satisfaction afterward. Common signs include noticeable hair loss, bald patches, uneven eyebrows or eyelashes, and behaviors like inspecting the pulled hair or rubbing it across the lips. Some individuals also engage in trichophagia, which is chewing or eating the pulled hair, increasing the risk of digestive complications.
Q: What causes trichotillomania?
A: The exact cause of trichotillomania is not fully understood, but it likely involves a combination of genetic, neurobiological, and environmental factors. Research suggests abnormalities in brain pathways related to impulse control and habit formation may play a role. Many people with trichotillomania have family members with similar behaviors or other body-focused repetitive behaviors. Stress, anxiety, and emotional regulation difficulties often contribute, though the behavior can also occur during relaxed or automatic states without conscious awareness.
A: Trichotillomania shares features with obsessive-compulsive disorder (OCD), such as repetitive behaviors and difficulty stopping despite negative consequences. It is classified in the same diagnostic category as OCD in the DSM-5, under obsessive-compulsive and related disorders. However, it is a distinct condition. While OCD behaviors are usually driven by intrusive thoughts and performed to reduce anxiety, hair pulling in trichotillomania may be motivated by sensory urges, emotional regulation, or habit, not necessarily by obsessions.
Q: Can trichotillomania lead to permanent hair loss or alopecia?
A: Repeated pulling can damage hair follicles over time, leading to thinning or permanent hair loss in affected areas. This type of hair loss is known as traction alopecia. In severe or long-standing cases, scar tissue may form, preventing new hair growth. Early intervention improves the chances of hair regrowth. Protecting the scalp and other areas from ongoing trauma is key to preventing irreversible damage.
Q: What are common triggers for hair-pulling episodes?
A: Triggers vary from person to person but often include stress, boredom, fatigue, or sitting in quiet environments like watching TV or studying. Some pull hair automatically, without realizing it, while others do so intentionally to manage emotions like anxiety or frustration. Physical sensations, such as an itchy scalp or uneven hair length, can also prompt pulling. Identifying personal triggers through journaling or behavioral tracking helps in developing effective coping strategies.
Q: What holistic or natural treatments can help manage trichotillomania?
A: Holistic approaches focus on reducing stress, improving self-awareness, and supporting emotional balance. Mindfulness practices, yoga, and breathing exercises help increase awareness of pulling urges and improve emotional regulation. Some people benefit from supplements like N-acetylcysteine (NAC), which may help reduce compulsive behaviors. Regular sleep, balanced nutrition, and physical activity support overall brain health and can reduce symptom severity. These methods work best when combined with behavioral therapy.
Q: Can acupuncture, hypnotherapy, or homeopathy help with trichotillomania?
A: Many individuals report improvement with complementary therapies like acupuncture, hypnotherapy, or homeopathy. Acupuncture may help by reducing anxiety and promoting relaxation. Hypnotherapy aims to access subconscious patterns and introduce new behavioral responses to pulling urges. Homeopathy uses highly diluted natural substances based on individual symptoms, but results vary widely and lack strong clinical support. These options may be considered as part of a broader treatment plan, especially when traditional methods are not fully effective.
Hypnosis for Trichotillomania at Philadelphia Hypnotherapy Clinic
You will receive specialized care at the Philadelphia Hypnotherapy Clinic to make your sessions go smoothly. In time, you can live free of your hair-pulling habit. It takes only courage to allow the hypnotherapist to enter your mind. Accepting the suggestions he makes represents an excellent achievement for the mind.
Dr. Tsan, the chief medical officer of the Philadelphia Hypnotherapy Clinic, has extensive experience in hypnosis, hypnotherapy, and neuro-linguistic programming. The treatment program for trichotillomania consists of three primary alternative techniques:
- Acupuncture for internal energy regulation and balancing
- Homeopathic remedies for urges reduction
- Hypnosis creates a healthy pattern in the patient’s subconscious mind.
Contact Philadelphia Hypnotherapy Clinic to book an appointment for an initial free consultation, and Dr. Tsan will personally discuss your particular case and the best treatment options.